Thyroid nodules are more common than most people realize. In fact, up to 67% of adults over 60 have them - often without knowing. Most are harmless, but a small percentage can be cancerous. The real challenge isn’t finding them - it’s knowing which ones need action and which ones can be left alone. Too many people end up with unnecessary surgeries because doctors don’t have clear guidance. Others miss real threats because they assume all nodules are harmless. The truth? It’s not about size alone. It’s about growth, appearance, and a few key numbers that tell you what’s really going on.
What Makes a Thyroid Nodule Suspicious?
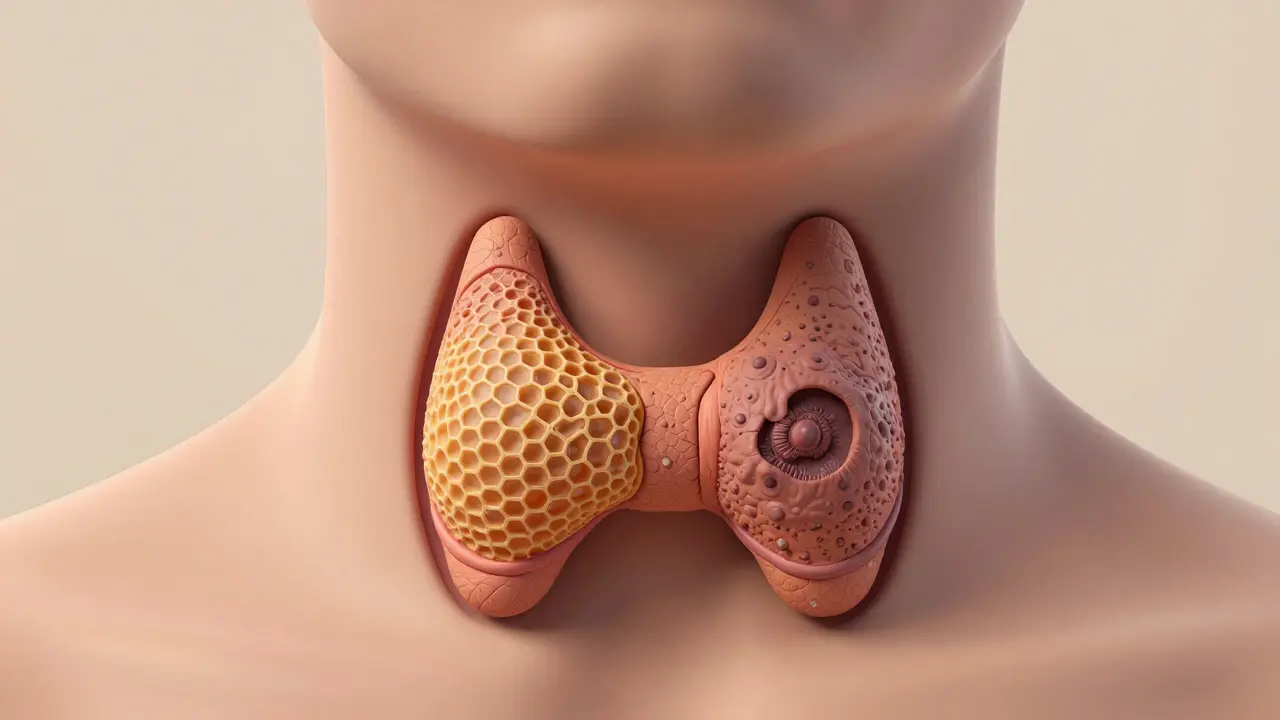
Not all thyroid nodules are the same. Some look like fluid-filled sacs. Others are solid lumps. The difference isn’t just in how they feel - it’s in how they look on an ultrasound. A benign nodule often has smooth edges, is filled with fluid, or has a spongy, honeycomb-like texture. These are almost always harmless. Cancerous ones? They tend to be solid, with jagged borders, tiny calcium deposits (called microcalcifications), and they appear darker than the surrounding tissue - what doctors call hypoechogenic.
These features aren’t guesses. They’re based on data from thousands of cases. For example, 83% of malignant nodules have irregular margins. 56% of papillary thyroid cancers - the most common type - show microcalcifications. And if a nodule is darker than the rest of the thyroid, that’s a red flag too. It’s not a diagnosis on its own, but when you see these signs together, the risk jumps.
Size Matters - But Not How You Think
You’ve probably heard that nodules larger than 1 cm need a biopsy. That’s true - but it’s not the whole story. A 1.5 cm nodule with smooth edges and no other warning signs might be perfectly fine. Meanwhile, a 7 mm nodule with microcalcifications and irregular borders could be cancer. Size is just one piece. The American Thyroid Association guidelines say biopsy is recommended if:
- The nodule is 1 cm or larger AND has suspicious ultrasound features
- The nodule is 1.5 cm or larger even without suspicious features
- The nodule is 2 cm or larger - no matter what it looks like
Why these numbers? Because research shows that below 1 cm, the chance of cancer is under 5%. But once you cross 2 cm, even if it looks calm on ultrasound, the risk climbs enough to warrant a closer look. The goal isn’t to biopsy everything. It’s to catch the ones that matter before they spread.
Growth Rate: The Silent Red Flag
Here’s something most people don’t know: how fast a nodule grows matters more than its size. A 2017 study in the Journal of Clinical Endocrinology & Metabolism found that if a nodule grows more than 2 mm per year in two dimensions, it’s significantly more likely to be cancerous. For every extra 2 mm/year beyond that, the risk keeps climbing.
Benign nodules barely budge. One five-year study found they grow, on average, just 1 mm per year. Only 14% of them even doubled in size. But cancerous ones? They don’t wait. If you had an ultrasound last year and your nodule grew from 1.1 cm to 1.5 cm - that’s 4 mm in 12 months. That’s a red flag. You don’t need to panic. But you do need a biopsy.
That’s why doctors now recommend serial ultrasounds - repeat scans every 6 to 12 months - for nodules that aren’t immediately biopsied. Tracking growth is now part of the standard. If it’s moving fast, you act. If it’s sitting still, you watch.
Benign vs. Cancerous: What’s Actually Inside?
Most benign nodules are one of three things: a colloid nodule (just built-up thyroid hormone storage), a follicular adenoma (a non-cancerous tumor), or a cyst (a fluid-filled sac). Pure cysts are almost always harmless. Even follicular adenomas - which look like cancer under a microscope - rarely turn into anything dangerous.
Cancerous nodules? Almost always papillary carcinoma - about 80% of cases. These grow slowly and often spread to nearby lymph nodes, but they’re highly treatable. The next most common is follicular carcinoma (10-15%), which doesn’t usually go to lymph nodes but can spread to lungs or bones. Rarer types - like medullary, anaplastic, or lymphoma - are uncommon but more aggressive.
What’s important here is this: most thyroid cancers are slow-growing and highly curable. The goal isn’t to remove every nodule. It’s to find the ones that could become dangerous if left alone.

When Is a Biopsy Really Necessary?
Biopsy - or fine-needle aspiration (FNA) - is the only way to know for sure. But not every nodule needs one. Here’s when it’s needed:
- Any nodule ≥1 cm with suspicious ultrasound features (irregular shape, microcalcifications, hypoechogenicity)
- Any nodule ≥1.5 cm, even if it looks normal
- Any nodule ≥2 cm - period
- Any nodule that grows more than 2 mm/year in two directions
- Any nodule with symptoms like trouble swallowing, breathing, or a persistent lump feeling
There’s also a gray zone: nodules in the 1-1.5 cm range with no clear signs. For these, doctors may wait and monitor - especially if the patient is young and healthy. But if growth kicks in, the biopsy happens.
And here’s the catch: 15-30% of initial biopsies come back as nondiagnostic. That means not enough cells were collected. The fix? Repeat the biopsy with ultrasound guidance. Success rates jump to 85-90% on the second try.
The Bethesda System: What the Lab Report Really Means
After a biopsy, the pathologist gives it a category - one of six levels called the Bethesda System. It’s not just a yes/no. It’s a risk scale:
| Category | Name | Malignancy Risk |
|---|---|---|
| 1 | Nondiagnostic | 1-4% |
| 2 | Benign | 0-3% |
| 3 | Atypia of Undetermined Significance | 5-15% |
| 4 | Follicular Neoplasm | 15-30% |
| 5 | Suspicious for Malignancy | 60-75% |
| 6 | Malignant | 97-99% |
Categories 1 and 2? Almost always safe. Category 6? Almost always cancer. The problem is categories 3 and 4 - the gray zone. That’s where molecular testing comes in.
Molecular Testing: Cutting Down Unnecessary Surgeries
Before 2020, if your biopsy came back as "atypia" or "follicular neoplasm," you were often told to get your thyroid removed. Why? Because the risk was too high to ignore. But now, tests like Afirma GSC and ThyroSeq v3 can analyze dozens of genes in the sample. They don’t just say "cancer" or "not cancer." They give you a probability.
ThyroSeq v3, approved by the FDA in 2022, looks at 112 genes. It has a 94% sensitivity - meaning it catches almost all cancers - and a 93% specificity - meaning it rarely flags harmless ones. A 2020 study showed these tests cut unnecessary surgeries by 35% in indeterminate cases.
Now, if you’re in category 3 or 4, your doctor might skip surgery entirely and just run the molecular test. If it says low risk? You go back to monitoring. If it says high risk? You proceed with surgery. No guesswork.

What About Overdiagnosis?
Here’s the uncomfortable truth: we’re finding way more thyroid cancers than we need to. Since 1975, thyroid cancer diagnoses have increased 15-fold - mostly because we’re scanning more. But many of these tumors are tiny, slow-growing, and would never cause harm. A 2021 study showed that 87% of microcarcinomas (under 1 cm) stayed the same over five years of monitoring.
That’s why experts now recommend active surveillance for very low-risk cancers. Instead of rushing to surgery, you get ultrasounds every 6-12 months. If it grows, you act. If it doesn’t, you leave it alone. This approach is gaining traction - and it’s saving thousands from unnecessary operations.
What Happens After a Biopsy?
If your biopsy says benign? You’re usually done. You might get one more ultrasound in 6-12 months to make sure nothing changed. If it’s suspicious or malignant? You’ll likely need surgery - either removing part of the thyroid (lobectomy) or the whole thing (thyroidectomy). After surgery, most people take daily thyroid hormone replacement. The prognosis is excellent: over 95% survival rate for papillary and follicular cancers.
If you’re told you need surgery, ask: "Is this because of cancer risk - or because of size and symptoms?" If it’s just big and uncomfortable, there are alternatives. Radiofrequency ablation - a minimally invasive procedure that heats and shrinks the nodule - is now being tested in clinical trials. Early results show it reduces volume by 78% in 12 months, with far fewer complications than surgery.
Who Should Be More Careful?
Women are three times more likely to develop thyroid nodules than men. Risk goes up with age - especially after 60. A history of radiation exposure (like childhood X-rays to the head or neck) raises your risk. So does a family history of thyroid cancer.
If you’re in any of these groups, be proactive. Don’t wait for symptoms. If you feel a lump, notice swelling, or have unexplained hoarseness or swallowing trouble - get checked. Ultrasound is quick, painless, and doesn’t use radiation. It’s the first step.
Final Takeaway
Thyroid nodules are common. Most are harmless. But ignoring them isn’t the answer. The key is knowing when to act. Focus on three things:
- Ultrasound features - irregular shape, microcalcifications, darkness
- Growth rate - more than 2 mm/year in two directions
- Size - ≥1 cm with suspicious features, ≥1.5 cm without, ≥2 cm always
Don’t let fear drive you to surgery. Don’t let complacency let you miss a real threat. Use the data. Ask for molecular testing if your biopsy is unclear. And if you’re told to wait - make sure you have a plan to check back.
Are all thyroid nodules cancerous?
No. In fact, over 90% of thyroid nodules are benign. Only about 5-10% turn out to be cancerous. Most are harmless fluid-filled cysts or slow-growing nodules that don’t cause problems.
Can a benign nodule turn cancerous?
It’s extremely rare. Benign nodules like follicular adenomas or colloid nodules don’t typically transform into cancer. The cancerous ones usually start as cancer from the beginning - they just weren’t detected until later.
Do I need a biopsy if my nodule is under 1 cm?
Not necessarily. If it’s under 1 cm and has no suspicious ultrasound features, most doctors will monitor it instead. But if it’s growing fast - more than 2 mm per year - even a small nodule may need a biopsy.
What does "atypia" mean on a biopsy report?
"Atypia of undetermined significance" (Category 3) means the cells look unusual but not clearly cancerous. The risk of cancer is 5-15%. Doctors usually recommend molecular testing or a repeat biopsy before deciding on surgery.
Can I avoid surgery if my nodule is cancerous?
For very small, low-risk papillary cancers (under 1 cm), active surveillance is now an option. You’ll get regular ultrasounds to monitor growth. If it stays stable, you may never need surgery. But for larger or more aggressive cancers, surgery is still the standard.
Robert Bliss
March 10, 2026 AT 04:43Katy Shamitz
March 10, 2026 AT 12:35Neeti Rustagi
March 10, 2026 AT 14:11rafeq khlo
March 12, 2026 AT 03:01Morgan Dodgen
March 14, 2026 AT 00:27Melba Miller
March 14, 2026 AT 13:28Judith Manzano
March 14, 2026 AT 23:01Janelle Pearl
March 15, 2026 AT 13:49Peter Kovac
March 15, 2026 AT 21:45Philip Mattawashish
March 17, 2026 AT 07:48Tom Sanders
March 18, 2026 AT 16:31Ray Foret Jr.
March 19, 2026 AT 11:24