PAD & Embolism Risk Assessment Tool
Risk Factor Assessment
Answer the following questions to assess your risk of developing PAD and embolism. This tool helps identify potential risk factors that may increase your likelihood of experiencing these conditions.
Your Current Health Status
Your Risk Assessment Results
Shared Risk Factors for Embolism and PAD
| Risk Factor | Effect on Atherosclerosis | Effect on Clot Formation |
|---|---|---|
| Smoking | Accelerates plaque buildup | Increases platelet activation |
| Diabetes | Damages vessel lining | Promotes hyper-coagulability |
| High LDL Cholesterol | Feeds plaque growth | Facilitates fibrin formation |
| Hypertension | Creates turbulent flow, fostering plaque | Triggers endothelial injury |
| Obesity | Inflammatory cytokines worsen atherosclerosis | Raises fibrinogen levels |
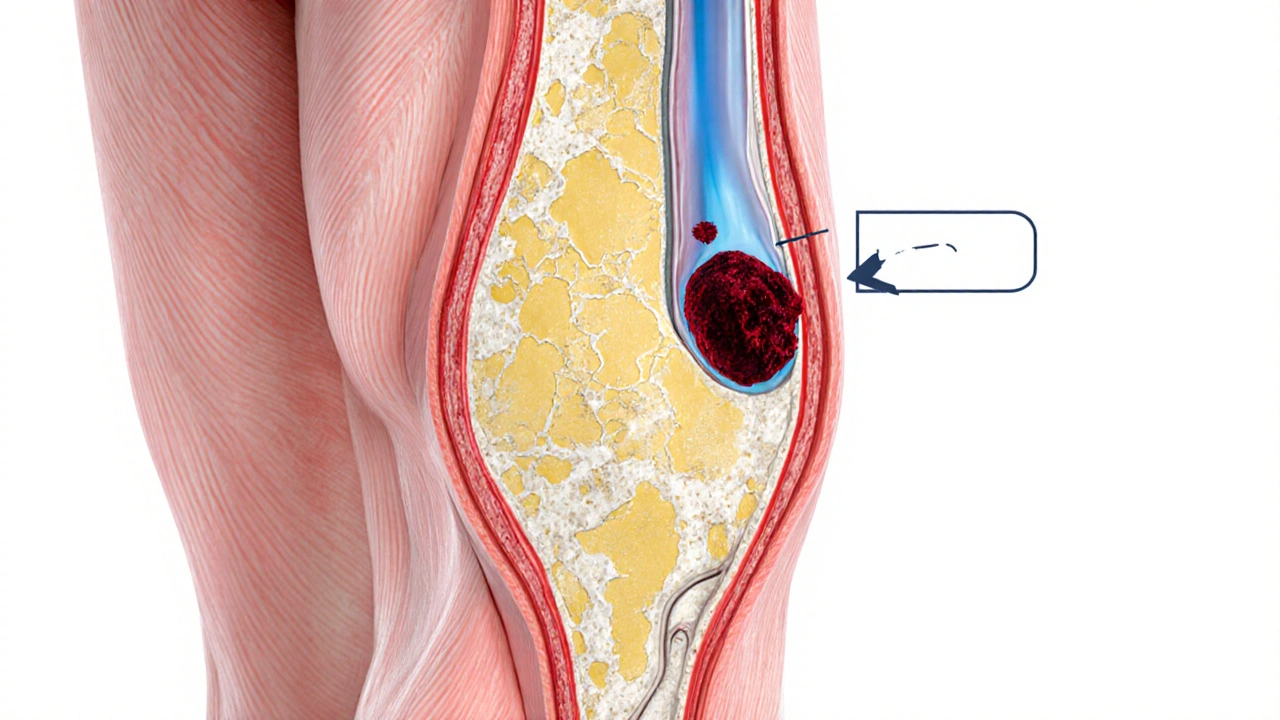
When a Embolism is a blockage of a blood vessel by a particle that has traveled from another part of the circulatory system, it can strike anywhere in the body. One of the places where it causes real trouble is the network of arteries that feed the legs and arms - the area affected by Peripheral Artery Disease (PAD). Understanding how these two conditions intersect helps you spot warning signs early, choose the right tests, and take steps to keep your limbs healthy.
What Is an Embolism? Types That Matter for PAD
Emboli come in several flavors, but the three most relevant to peripheral circulation are:
- Thrombo‑emboli: clots that break off from a larger thrombus, often forming in the heart or a diseased artery.
- Fat emboli: tiny fat droplets that can travel after a bone fracture.
- Air emboli: pockets of air entering the bloodstream, usually during invasive procedures.
For PAD patients, the first type-thrombo‑emboli-is the chief villain because a clot can lodge in already narrowed leg arteries, worsening the flow restriction caused by atherosclerosis.
Peripheral Artery Disease Explained
Peripheral Artery Disease is a progressive narrowing of the arteries outside the heart and brain, most often due to atherosclerosis, the buildup of fatty plaques inside vessel walls.
Typical symptoms include:
- Claudication - cramping pain when walking that eases with rest.
- Rest pain - persistent discomfort, usually at night.
- Non‑healing ulcers or gangrene on the toes or feet.
When an embolism adds another blockage, these symptoms can flare up suddenly, turning chronic discomfort into an emergency.
How an Embolism Triggers a PAD Flare‑Up
Imagine a road already narrowed by construction (the atherosclerotic plaque). A sudden traffic jam (the embolus) blocks the remaining lane, halting all flow. In the body, the embolus can:
- Increase the pressure gradient across the narrowed segment, amplifying pain.
- Reduce oxygen delivery (Ischemia), leading to tissue damage faster than the body can compensate.
- Prompt the body’s clot‑breaking mechanisms, which can cause further fragmentation and more tiny emboli.
The result is an abrupt worsening of claudication, new rest pain, or even sudden foot discoloration-a sign of critical limb ischemia.
Key Risk Factors Shared by Embolism and PAD
Both conditions thrive on the same unhealthy habits and medical issues. Knowing them helps you lower the odds of a dangerous overlap.
| Risk Factor | Effect on Atherosclerosis | Effect on Clot Formation |
|---|---|---|
| Smoking | Accelerates plaque buildup | Increases platelet activation |
| Diabetes | Damages vessel lining | Promotes hyper‑coagulability |
| High LDL Cholesterol | Feeds plaque growth | Facilitates fibrin formation |
| Hypertension | Creates turbulent flow, fostering plaque | Triggers endothelial injury |
| Obesity | Inflammatory cytokines worsen atherosclerosis | Raises fibrinogen levels |
How Doctors Diagnose an Embolism in a PAD Patient
Because the symptoms overlap, a careful work‑up is essential.
- Ankle‑Brachial Index (ABI): A simple ratio of ankle to arm blood pressure. Values below 0.9 suggest PAD; a sudden drop can hint at an acute embolic event.
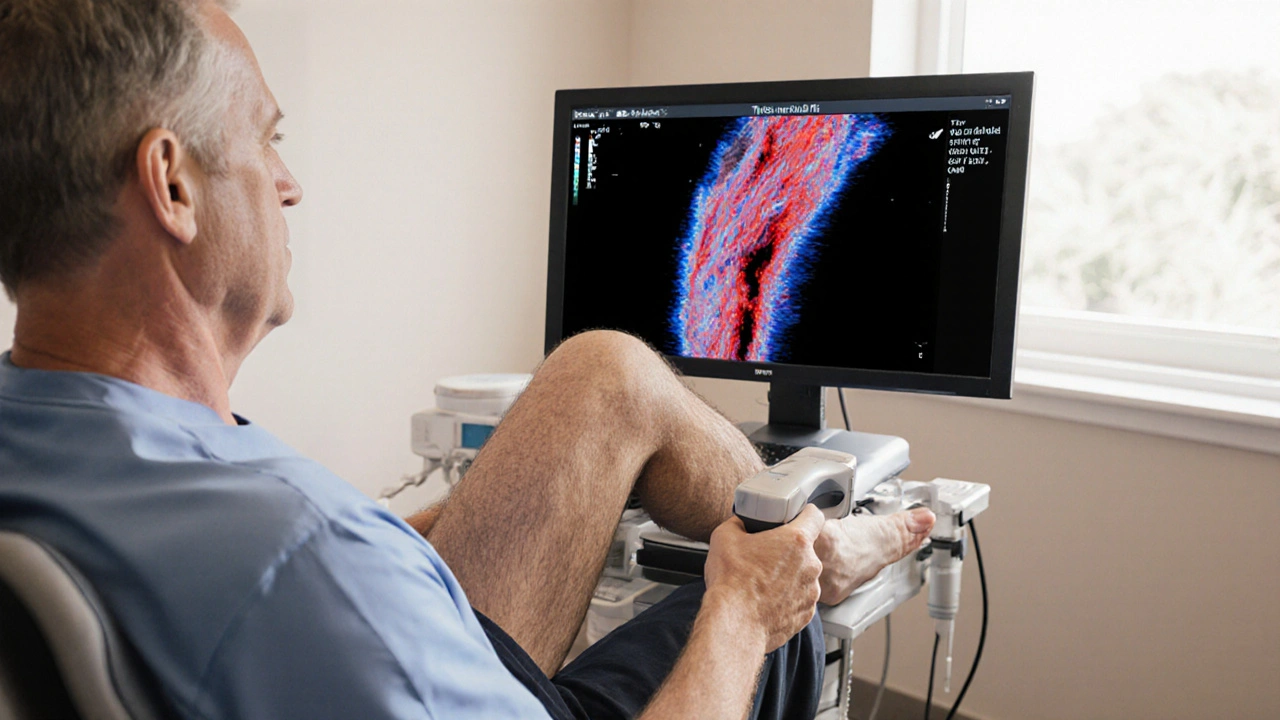
- Duplex Ultrasound: Visualizes blood flow and can spot a moving clot within the artery.
- Computed Tomography Angiography (CTA) or Magnetic Resonance Angiography (MRA): Provide detailed images of vessel blockage and can differentiate plaque from an embolus.
- Blood Tests: D‑dimer levels rise in active clotting; elevated C‑reactive protein points to inflammation.
When an embolus is identified, the treatment pathway shifts quickly toward clot‑removal or dissolution.
Treatment Strategies: Tackling Both the Clot and the Underlying PAD
Effective care attacks the problem on two fronts: clearing the embolus and improving the long‑term arterial health.
Acute Embolism Management
- Anticoagulants (e.g., heparin, rivaroxaban) - thin the blood to prevent the clot from growing.
- Thrombolytic therapy - drugs like alteplase dissolve the clot, used when the blockage threatens limb viability.
- Catheter‑directed embolectomy - a minimally invasive procedure that physically extracts the clot.
Long‑Term PAD Care
- Antiplatelet agents such as aspirin or clopidogrel reduce new plaque‑related clots.
- Statin therapy lowers LDL cholesterol and stabilizes existing plaques.
- Angioplasty with stent placement - opens the narrowed artery and provides structural support.
- Bypass surgery - creates a new route for blood flow around severe blockages.
- Lifestyle changes: regular walking program, smoking cessation, balanced diet low in saturated fats, and strict blood‑pressure control.
Combining medication with a supervised exercise regimen can improve walking distance by up to 200 meters within three months, according to recent vascular studies.
When to Seek Immediate Medical Help
If you notice any of these red‑flag signs, call emergency services right away:
- Sudden, severe leg pain that doesn’t ease with rest.
- Pale or bluish skin on a foot or toe, especially if it’s cold to the touch.
- Rapidly spreading ulcer or open wound.
- Unexplained weakness or loss of sensation in the leg.
These symptoms could signal a critical embolic event that threatens tissue survival.
Preventing Future Embolism‑PAD Interactions
Prevention is a blend of medical vigilance and daily habits.
- Schedule regular vascular check‑ups if you have diabetes, high blood pressure, or a smoking history.
- Adhere to prescribed antiplatelet or anticoagulant regimens-missing doses raises clot risk dramatically.
- Monitor your cholesterol; aim for LDL below 70mg/dL if you’ve already been diagnosed with PAD.
- Stay active: a daily 30‑minute walk keeps arteries flexible and encourages collateral circulation.
- Maintain a healthy weight; each 5kg of excess adds roughly a 10% increase in clot‑formation risk.
By addressing the shared risk landscape, you lower the chance that an embolus will ever find a weak spot in a peripheral artery.
Frequently Asked Questions
Can an embolism cause a heart attack?
Yes. If a clot travels from a peripheral vein to the coronary arteries-a rare event called a coronary embolism-it can block blood flow and trigger a heart attack.
Is PAD only a problem for older adults?
While prevalence rises after age 60, younger people with diabetes, smoking habits, or a strong family history can develop PAD early.
What’s the difference between a clot and an embolus?
A clot (thrombus) forms in place; an embolus is that clot-or a piece of it-dislodged and traveling through the bloodstream.
Can exercise worsen a blockage caused by an embolus?
Mild activity improves circulation, but intense exertion may increase pain if the embolus sharply limits blood flow. Follow your doctor’s guidance on safe activity levels.
How long does it take for a clot‑removing procedure to restore limb function?
Most patients experience noticeable symptom relief within hours after successful embolectomy or thrombolysis, although full recovery may take weeks of rehab.
Darla Sudheer
October 8, 2025 AT 16:08Thanks for the thorough overview; the risk tool looks handy.
Elizabeth González
October 12, 2025 AT 03:28The article provides a comprehensive synthesis of the pathophysiological mechanisms linking embolic events to peripheral artery disease. The inclusion of a self‑assessment questionnaire is particularly valuable for clinicians seeking to stratify patient risk. However, the methodological limitations of the risk scoring algorithm warrant further clarification.
chioma uche
October 15, 2025 AT 14:48Our people are being misled by foreign medical journals that downplay the impact of lifestyle on PAD; the real killer is the Western diet that floods our arteries with junk. If we don’t stand up and demand stricter regulations on tobacco and processed foods, the epidemic will keep crushing our nation.
Satyabhan Singh
October 19, 2025 AT 02:08From a South Asian perspective, the interplay between hyperglycaemia and endothelial dysfunction is accentuated by traditional dietary patterns rich in refined carbohydrates. Incorporating culturally appropriate interventions, such as increased consumption of millet and fenugreek, may ameliorate both atherosclerotic progression and thrombotic propensity.
Keith Laser
October 22, 2025 AT 13:28Oh great, another risk calculator-just what we needed to spend our evenings filling out forms instead of living our lives. If you’re looking for motivation, remember that every extra step you take is a tiny victory against the clot machine, so keep marching, folks.
Winnie Chan
October 26, 2025 AT 00:48Sure, because nothing says “fun Friday night” like clicking a bunch of radio buttons about smoking and cholesterol. At least the tool finally admits that walking 30 minutes isn’t just a suggestion, it’s a lifesaver.
Kyle Rensmeyer
October 29, 2025 AT 11:08Look at this risk tool it’s just another way for pharma to push pills lol they never tell you about the hidden chemicals in the water that make clots form faster 😒 the whole system is rigged and we’re the ones paying the price
Rod Maine
November 1, 2025 AT 22:28Thiss tool is realy helpful but i think it could be beter if it woudln't be so comlexh to use. Maybe add more colors so its more funy.
Othilie Kaestner
November 5, 2025 AT 09:48While the data presented is solid, I’d argue that focusing solely on individual risk factors overlooks the broader socioeconomic determinants that drive PAD prevalence. Without addressing access to healthy foods and safe walking spaces, any calculator is just a band‑aid.
Sebastian Samuel
November 8, 2025 AT 21:08👍 Absolutely, the checklist is a solid start! 💪 But remember, it’s just one piece of the puzzle – lifestyle changes are the real game‑changer. 🌿🏃♂️
Mitchell Awisus
November 12, 2025 AT 08:28First, the correlation between embolic phenomena and peripheral artery disease is well‑established in the literature, and this article does a commendable job of summarizing the key mechanisms. Second, the inclusion of a risk assessment tool offers practical value for both clinicians and patients alike; however, its predictive accuracy remains to be validated in larger cohorts. Third, smoking emerges as a dominant modifiable factor, accelerating plaque formation and platelet activation, which underscores the need for robust cessation programs. Fourth, diabetes is highlighted not only for its metabolic impact but also for its role in endothelial damage, amplifying thrombogenic potential. Fifth, the discussion of high LDL cholesterol ties lipid management directly to fibrin formation, reinforcing current statin guidelines. Sixth, hypertension’s contribution via turbulent flow is a reminder that blood pressure control must be aggressive and multifaceted. Seventh, obesity is linked to inflammatory cytokines, a pathway that may be mitigated through dietary interventions. Eighth, while the questionnaire asks about physical activity, it stops short of offering tailored exercise prescriptions, which could enhance its utility. Ninth, family history is mentioned, yet genetic testing is not explored despite emerging evidence of hereditary clotting disorders. Tenth, the article could benefit from a deeper dive into antithrombotic therapy options for high‑risk individuals. Eleventh, patient education remains a cornerstone; the tool should integrate educational modules to improve adherence. Twelfth, the authors wisely note the importance of regular follow‑up, but practical scheduling strategies are omitted. Thirteenth, the web‑based interface appears user‑friendly, yet mobile compatibility issues may limit accessibility for older patients. Fourteenth, future research directions could include machine‑learning algorithms to refine risk scoring. Fifteenth, overall, this piece bridges pathophysiology and actionable assessment, but its impact will depend on rigorous external validation and integration into clinical workflows.
Annette Smith
November 15, 2025 AT 19:48Great resource, very clear.
beth shell
November 19, 2025 AT 07:08The systematic presentation of shared risk factors offers a valuable educational framework, and I appreciate the balanced tone that encourages proactive health measures without inducing undue alarm.
khushali kothari
November 22, 2025 AT 18:28From a hemodynamic perspective, the synergistic interplay between shear stress alterations and platelet aggregation cascades underpins the pathogenesis of embolic events in PAD, necessitating a nuanced approach to antiplatelet pharmacotherapy that accounts for pharmacokinetic variability and receptor polymorphisms.
Brandon Smith
November 26, 2025 AT 05:48It is incumbent upon each of us to reject complacency and demand that healthcare systems prioritize preventive measures over profit‑driven interventions; ignoring the clear link between lifestyle choices and vascular health is simply unethical.
darwin ambil
November 29, 2025 AT 17:08💡 Good point! Adding a reminder to schedule annual vascular check‑ups would make the tool even more comprehensive. 📅👍
Kelvin Van der Maelen
December 1, 2025 AT 15:08Behold! The silent assassin in our veins strikes when we least expect it, and this article shines a blinding spotlight on the villainous culprits that conspire against our very lifeblood!