Anticoagulant Safety Calculator for Spinal Procedures
Calculate Safe Anticoagulant Timing
This tool helps determine when to stop and restart anticoagulants before spinal procedures based on ASRA guidelines. Accurate timing is critical to prevent spinal epidural hematoma.
Safety Timing Recommendations
Stop Anticoagulant:
Restart Anticoagulant:
ASRA Guidelines: Always confirm with your medical team. These recommendations are based on 2022 ASRA guidelines.
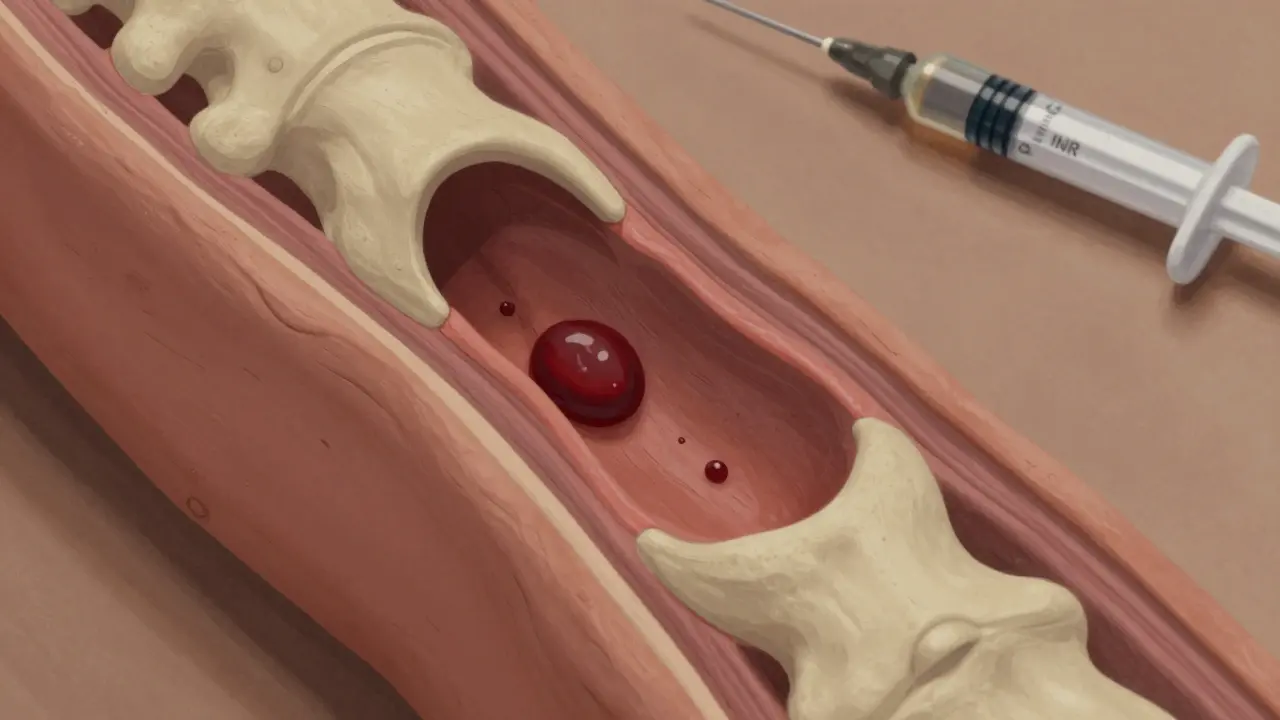
When you're on blood thinners and need an epidural or spinal procedure-whether for labor, chronic back pain, or surgery-the biggest fear isn't the needle. It's the hematoma. A single drop of blood trapped in the tight space around your spinal cord can lead to permanent paralysis. This isn't a rare nightmare. It's a documented risk that happens more often than most patients and even some doctors realize.
What Exactly Is a Spinal Epidural Hematoma?
A spinal epidural hematoma (SEH) is a collection of blood that forms between the dura mater (the tough outer membrane covering the spinal cord) and the ligamentum flavum (a ligament in your spine). This space is tiny-less than a teaspoon in volume. Just 1 to 2 milliliters of blood can crush the spinal cord. The result? Numbness, weakness, loss of bladder control, and sometimes complete paralysis. The scary part? Symptoms can show up within hours. Back pain, tingling in the legs, or sudden difficulty moving your feet aren't normal after an epidural. They're red flags. Studies show that if you don't get surgery within 8 hours of symptoms starting, your chance of full recovery drops from 79% to just 9%. Delayed treatment can mean living with permanent nerve damage.Which Blood Thinners Are Most Dangerous?
Not all anticoagulants are the same when it comes to spinal procedures. The risk depends on the drug, the dose, and how long it's been since your last dose.- Warfarin: The old standard. If your INR (a blood test that measures clotting time) is above 1.4, your risk jumps 8.7 times. Even if your INR is "normal" (1.2), there are documented cases of hematomas. Always check your INR within 24 hours before the procedure. Wait at least 4 hours after a single-shot epidural to restart it.
- Low Molecular Weight Heparin (LMWH): Drugs like Lovenox (enoxaparin) are common after hip or knee surgery. If you take a therapeutic dose, you need to wait 24 hours after your last injection before the procedure. Prophylactic doses still require a 10-12 hour wait. Restarting too soon-within 2 hours after a single shot, or 4 hours after a catheter-is a leading cause of preventable harm.
- Direct Oral Anticoagulants (DOACs): These include Xarelto (rivaroxaban), Eliquis (apixaban), and others. For people with normal kidney function, stop Xarelto or Eliquis at least 48 hours before the procedure. If your kidneys aren't working well (CrCl under 50 mL/min), wait 72 hours. Even then, cases have happened after following these rules. That’s why timing isn’t just a suggestion-it’s a safety line.
- Antiplatelets: Aspirin alone? Risk is extremely low-under 0.03%. But if you're on dual therapy-like aspirin plus clopidogrel-your risk triples. Many doctors still hold these drugs for 7 days before spinal procedures, but evidence is mixed. Some studies show no harm continuing aspirin; others report paralysis after stopping clopidogrel for only 3 days.
Who’s at Highest Risk?
It’s not just about the drug. Your body matters too. Here are the real risk factors, backed by data:- Age over 70: Your blood vessels become more fragile. Risk jumps 3.7 times.
- Chronic kidney disease: If your creatinine clearance is under 30 mL/min, your body can't clear anticoagulants properly. Risk goes up nearly 5 times.
- Spinal stenosis or scoliosis: These narrow your spinal canal. Even a small hematoma can compress the cord. Risk doubles.
- Multiple needle attempts: If the anesthesiologist has to poke you three or more times, your risk spikes 6.2 times. Traumatic puncture-with blood in the spinal fluid-raises risk 11.8 times.
- Epidural catheter vs. single shot: Leaving a catheter in place increases risk 2.3 times. That’s why many clinics now prefer single injections for pain management.
- Low hemoglobin or heavy bleeding: If your blood count is under 10 g/dL or you lose more than 1 liter of blood during surgery, your risk doubles or triples.

What Do the Guidelines Actually Say?
The American Society of Regional Anesthesia and Pain Medicine (ASRA) updates its guidelines every few years. Their 2017 recommendations are still the gold standard. But here’s the catch: many providers don’t follow them. A 2022 survey of 345 pain doctors found only 58% knew the correct timing for all anticoagulants. And 27% had experienced a near-miss-where a patient almost developed a hematoma because someone missed a window. The ASRA guidelines are clear:- Check INR within 24 hours before warfarin procedures. Target: under 1.4.
- Hold LMWH 10-12 hours for prophylaxis, 24 hours for treatment.
- Hold DOACs 48 hours (normal kidneys), 72 hours (impaired kidneys).
- Don’t restart anticoagulants until 2-4 hours after a single injection, or 4-6 hours after a catheter is removed.
- Document everything. The FDA found 34% of Lovenox-related hematomas happened because the patient’s anticoagulant status wasn’t recorded properly.
Real Stories Behind the Numbers
Statistics don’t tell the whole story. In a 2018 case report, a 68-year-old woman had a hip replacement. She was on rivaroxaban. Her doctors held it for 48 hours. She got her epidural. Everything looked fine. Twelve hours later, she lost feeling in her saddle area-her groin, buttocks, inner thighs. She had a spinal hematoma. Emergency surgery happened within 6 hours. She still ended up with permanent nerve damage in her left leg. On Reddit, an anesthesiologist shared a near-miss: a patient on therapeutic enoxaparin developed sudden leg weakness after an epidural catheter was removed. The team caught it early. They rushed her to MRI, found the hematoma, and operated within 5 hours. She recovered fully. That’s the difference between a protocol followed and one ignored.
Why This Matters More Than Ever
In 2022, over 40 million spinal procedures were done in the U.S. alone. Millions of those patients are on anticoagulants. The global anticoagulant market is worth over $23 billion. And the cost of one spinal hematoma? Around $287,000-mostly from long-term rehab and care for permanent disability. The FDA now requires a Risk Evaluation and Mitigation Strategy (REMS) for all anticoagulants. That means prescribers must be trained on these risks. Hospitals are being monitored. Starting in 2025, any U.S. hospital doing more than 50 spinal procedures a year must report SEH prevention metrics-or face penalties.What Should You Do?
If you’re on blood thinners and scheduled for an epidural or spinal procedure:- Know exactly which drug you’re taking-and the dose.
- Ask your doctor: "What’s the exact timing for stopping and restarting?" Don’t assume.
- Request an INR test if you’re on warfarin. Make sure it’s done within 24 hours of your procedure.
- Ask if you can have a single-shot epidural instead of a catheter. Lower risk.
- Report any back pain, numbness, or loss of bladder control immediately after the procedure. Don’t wait.
- Ask for a copy of the ASRA checklist. Many clinics use it now.
Pankaj Singh
January 13, 2026 AT 03:56This post is pure gold. But let’s be real-most hospitals don’t give a damn about ASRA guidelines. I’ve seen nurses restart Lovenox 3 hours after catheter removal because the chart didn’t say ‘hold.’ And guess who gets paralyzed? The patient. This isn’t negligence-it’s systemic laziness. The FDA’s new penalties won’t fix this. Only lawsuits will. And they’re coming.
Angel Molano
January 15, 2026 AT 00:38Stop. Just stop. If you’re on blood thinners and need an epidural, you don’t get to be lazy. 48 hours isn’t a suggestion-it’s your last chance to keep walking. If your doctor doesn’t know this, fire them.
Vinaypriy Wane
January 16, 2026 AT 20:57I just had a spinal fusion last month-on rivaroxaban. My anesthesiologist pulled out the ASRA checklist like it was a sacred text. She checked my INR, asked about kidney function, even had me sign a form acknowledging the risks. It felt overwhelming… but safe. If you’re reading this and you’re nervous? Ask for that checklist. Don’t be shy. Your spine is worth it.
Diana Campos Ortiz
January 18, 2026 AT 17:26my dr told me to stop xarelto 48hrs before… but i forgot to tell him i was also on aspirin. i was so scared. but he checked everything before the epidural and we did a single shot instead of a catheter. i’m fine now. but please… talk to your team. even if it feels awkward.
laura Drever
January 20, 2026 AT 09:42eh i dont care. i got my epidural on clexane and lived. stop scaremongering.
jefferson fernandes
January 20, 2026 AT 13:02Let’s not forget the human element here. Anesthesiologists are overworked. Nurses are understaffed. Patients are anxious. But the data doesn’t lie: multiple needle sticks, delayed diagnosis, and poor documentation are the real killers-not the drugs themselves. We need better protocols, yes-but we also need better communication. Ask for a timeout before the procedure. Demand that someone reads back the anticoagulant status. Make it a ritual. Because one missed detail… is one life changed forever.
James Castner
January 22, 2026 AT 06:34Consider the metaphysical weight of this issue: the human body is a vessel of exquisite vulnerability. A single milliliter of blood, misplaced by a fraction of a centimeter, can sever the thread between autonomy and dependence. We have advanced to the point where we can manipulate coagulation cascades with molecular precision, yet we still rely on paper checklists and human memory to prevent catastrophe. Is this not the paradox of modern medicine? We possess the knowledge to prevent suffering-but we lack the systemic humility to enforce it consistently. The ASRA guidelines are not merely clinical recommendations; they are moral imperatives written in the language of neurology and physiology. To ignore them is not negligence-it is a betrayal of the covenant between healer and healed. The cost of a hematoma is not measured in dollars, but in the silence of a body that can no longer answer the call of its own will.
Adam Rivera
January 22, 2026 AT 14:18Hey everyone-just wanted to say thanks for this thread. I’m from India, and we don’t talk about this stuff enough. My dad had a spinal procedure last year on warfarin. He’s fine now, but we almost lost him because the local doc didn’t check the INR. I printed out the ASRA chart and gave it to his team. Now I’m telling everyone I know: ask questions. Don’t be polite if your life’s on the line. You got this.